Abstract
Introduction: Total Body Irradiation (TBI) remains a crucial preparatory regimen for hematopoietic stem cell transplantation. However, traditional techniques involve complex workflows requiring dual CT simulations-Head-First Supine (HFS) and Feet-First Supine (FFS)-which pose logistical, dosimetric, and patient comfort challenges. This study introduces a simplified TBI approach using a single HFS CT scan combined with Surface Guided Radiation Therapy (SGRT) for setup verification and intra-fraction motion monitoring on the Radixact® TomoTherapy system. Materials and Methods: From August 2024 to April 2025, five adult patients with hematologic malignancies scheduled for TBI were retrospectively analyzed. Each patient underwent a single HFS simulation scan on PET-CT with full-body coverage. Immobilization was achieved using a vacuum cushion and thermoplastic mask. Treatment planning was performed using Accuray Precision® version 3.5.0.2 on a single CT dataset. Two helical plans, one for the upper body and one for the lower body, were generated with a 14 cm overlap at the mid-thigh. Seven feathered Planning Target Volumes (PTVs) were created at the junction to ensure dose homogeneity. Surface Guided Radiation Therapy (SGRT) was used for initial setup and intra-fraction motion monitoring, while ClearRT-based kVCT imaging served as a secondary internal verification. Patient-specific quality assurance (PSQA) was conducted using Delta4 with 3%/3 mm gamma criteria, and junction dose validation was performed using ion chamber measurements. Results: SGRT enabled accurate patient setup for TBI, with mean translational errors ≤2 mm and rotational errors ≤0.6° when compared to kVCT verification. Real-time motion monitoring during treatment enabled automatic beam-holds with an average latency of 0.0038 seconds, ensuring precise delivery. Dosimetric results showed excellent target coverage (≥95% of the PTV receiving ≥95% of the prescribed dose) and homogeneous dose distribution. Smooth dose profiles were observed at plan junctions, and lung doses remained within safe limits (~1.7 Gy). Pre-treatment QA demonstrated high gamma pass rates across all body regions (mean ≥96.6%), confirming treatment accuracy. Discussion: This simple modified workflow utilizing a single HFS CT scan for full-body TBI on Radixact eliminates the need for patient repositioning and FFS imaging, thereby simplifying the planning and delivery process. Integration of SGRT provides non-ionizing, real-time monitoring, enhancing setup precision and intra-fraction control. The feathered PTV junction design effectively mitigated dose inhomogeneities. This method demonstrates not only dosimetric robustness but also improved workflow efficiency and patient comfort.
Keywords
Total Body Irradiation, TBI, SGRT, Radiaxact, Tomotherapy, Single CT, Tomohelical, VoloUltra
1. Introduction
Total Body Irradiation (TBI) is a cornerstone in preparative regimens for hematopoietic stem cell transplantation, primarily aimed at eliminating residual malignant cells and inducing immunosuppression to facilitate engraftment
| [1] | Gruen A, Ebell W, Wlodarczyk W, et al.: Helical tomotherapy for total body irradiation - a prospective study of dosimetric quality, feasibility, and acute toxicity. Radiat Oncol. 20138, 92-10. https://doi.org//10.1186/1748-717X-8-92 |
| [2] | Khan FM, Gibbons JP: The Physics of Radiation Therapy. Philadelphia, PA: Lippincott Williams & Wilkins; 2014. |
| [3] | Halperin EC, Constine LS, Tarbell NJ, Kun LE: Pediatric Radiation Oncology. Philadelphia, PA. Lippincott Williams & Wilkins, 2010. https://link.springer.com/content/pdf/10.1007/978-3-319-43545-9.pdf |
[1-3]
. Traditionally, TBI was delivered using simple setups involving large parallel-opposed beams at extended source-to-skin distances (SSDs)
| [4] | Heublein AC. A: Preliminary report on continuous irradiation of the entire body. Radiology. 193218, 1051-1062. https://doi.org/10.1148/18.6.1051 |
| [5] | Deeg HJ, Sullivan KM, Buckner CD, et al.: Marrow transplantation for acute nonlymphoblastic leukemia in first remission: toxicity and long-term follow-up of patients conditioned with single dose or fractionated total body irradiation. Bone Marrow Transplant. 1986, 1: 151-157. |
| [6] | Girinsky T, Benhamou E, Bourhis JH, et al.: Prospective randomized comparison of single-dose versus hyperfractionated total-body irradiation in patients with hematologic malignancies. J Clin Oncol. 200018, 981-986. https://doi.org/10.1200/JCO.2000.18.5.981 |
| [7] | Van Dyk J, Galvin J, Glasgow G, Podgorsak E: AAPM Report No. 17. The physical aspects of total and half body photon irradiation. New York: American Association of. Physicists in Medicine. 1986. |
[4-7]
. While effective in coverage, these setups often resulted in uneven dose distribution and limited protection of normal tissues. The inability to adequately spare critical organs led to substantial dose inhomogeneities and associated toxicities
| [5] | Deeg HJ, Sullivan KM, Buckner CD, et al.: Marrow transplantation for acute nonlymphoblastic leukemia in first remission: toxicity and long-term follow-up of patients conditioned with single dose or fractionated total body irradiation. Bone Marrow Transplant. 1986, 1: 151-157. |
[5]
.
With technological advancements, modern radiotherapy techniques such as three-dimensional conformal radiotherapy (3DCRT), Intensity-Modulated Radiation Therapy (IMRT), and later, Volumetric Modulated Arc Therapy (VMAT), have progressively been employed to enhance treatment accuracy and minimize exposure to organs at risk (OARs)
| [8] | Chretien M, Cote C, Blais R, et al.: A variable speed translating couch technique for total body irradiation. Med Phys. 200027, 1127-1130. https://doi.org/10.1118/1.598978 |
| [9] | Brown DW, Knibutat K, Edmonds N, et al.: A novel translational total body irradiation technique. J Med. 2010031003, https://doi.org/10.1115/1.4001864 |
| [10] | Hussain A, Villarreal-Barajas JE, Dunscombe P, Brown DW: Aperture modulated, translating bed total body irradiation. Med Phys. 201138, 932-941. https://doi.org//10.1118/1.3534196 |
| [11] | Springer A, Hammer J, Winkler E, et al.: Total body irradiation with volumetric modulated arc therapy: dosimetric data and first clinical experience. Radiat Oncol. 201611, 46. https://doi.org/10.1186/s13014-016-0625-7 |
| [12] | Tas B, Durmus IF, Okumus A, et al.: Total-body irradiation using linac-based volumetric modulated arc therapy: Its clinical accuracy, feasibility and reliability. Radiother Oncol. 2018: 527-533. https://doi.org/10.1016/j.radonc.2018.08.005 |
| [13] | Ouyang L, Folkerts M, Zhang Y, et al.: Volumetric modulated arc therapy based total body irradiation: Workflow and clinical experience with an indexed rotational immobilization system. Phys Imaging Radiat Oncol. 20174, 22-25. https://doi.org/10.1016/j.phro.2017.11.002 |
[8-13]
. Among these, VMAT and RapidArc have allowed for more conformal and efficient dose delivery to the entire body or specific marrow compartments, resulting in better organ preservation and improved therapeutic ratios
| [14] | Köksal M., Özkan O., Holderried T, et al.: Optimized conformal total body irradiation with VMAT using a linear-accelerator-based radiosurgery treatment system in comparison to the golden standard helical TomoTherapy. Cancers. 202315. https://doi.org/10.3390/cancers15174220 |
| [15] | Thanvi S, Shinde R, Chandar H, et al.: Dosimetric comparison of VMAT vs 3DCRT in TBI using single HFS CT scan with anterior-posterior/posterior-anterior (AP/PA) field matching in cranial and caudal junctions. Asian Pac J Cancer Care. 2024: 49-53. https://doi.org/10.31557/APJCC.2024.9.1.49-53 |
| [16] | J P Cleuziou, C. Desgranges, I. Henry, et al.: Total body irradiation using helical tomotherapy: Set-up experience and in-vivo dosimetric evaluation. Cancer Radiother. 202125, 213-221. https://doi.org/10.1016/j.canrad.2020.07.009 |
[14-16]
.
Helical tomotherapy, including the newer Radixact® system, represents a significant innovation in TBI delivery. These systems offer continuous helical radiation delivery, achieving excellent dose uniformity and more individualized sparing of sensitive organs
| [1] | Gruen A, Ebell W, Wlodarczyk W, et al.: Helical tomotherapy for total body irradiation - a prospective study of dosimetric quality, feasibility, and acute toxicity. Radiat Oncol. 20138, 92-10. https://doi.org//10.1186/1748-717X-8-92 |
| [17] | Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279. https://doi.org/10.1016/j.ijrobp.2008.04.071 |
| [18] | Susanta K. Hui, Jeff Kapatoes, Jack Fowler, et al.: Feasibility study of helical tomotherapy for total body or total marrow irradiation. Med Phys. 200532, 3214: 3224. https://doi.org/10.1118/1.2044428 |
| [19] | V. Sarradin, L. Simon, A. Huynh, et al.: Total body irradiation using Helical Tomotherapy®: Treatment technique, dosimetric results and initial clinical experience. Cancer Radiother. 201822, 17-24. https://doi.org/10.1016/j.canrad.2017.06.014 |
| [20] | S. R. Faught, S. Y. Firat, C. A. Lawton, et al.: A Dosimetric Comparison of Conventional Radiotherapy and Helical Tomotherapy (HT) for Total Body Irradiation (TBI). Int J Radiat Oncol Biol. 200872, https://doi.org/10.1016/j.ijrobp.2008.06.1452 |
[1, 17-20]
. Numerous studies have confirmed the clinical applicability and dosimetric benefits of tomotherapy in TBI, highlighting reductions in pulmonary and renal toxicity compared to earlier methods
| [17] | Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279. https://doi.org/10.1016/j.ijrobp.2008.04.071 |
| [18] | Susanta K. Hui, Jeff Kapatoes, Jack Fowler, et al.: Feasibility study of helical tomotherapy for total body or total marrow irradiation. Med Phys. 200532, 3214: 3224. https://doi.org/10.1118/1.2044428 |
| [19] | V. Sarradin, L. Simon, A. Huynh, et al.: Total body irradiation using Helical Tomotherapy®: Treatment technique, dosimetric results and initial clinical experience. Cancer Radiother. 201822, 17-24. https://doi.org/10.1016/j.canrad.2017.06.014 |
| [20] | S. R. Faught, S. Y. Firat, C. A. Lawton, et al.: A Dosimetric Comparison of Conventional Radiotherapy and Helical Tomotherapy (HT) for Total Body Irradiation (TBI). Int J Radiat Oncol Biol. 200872, https://doi.org/10.1016/j.ijrobp.2008.06.1452 |
[17-20]
. Additionally, the emergence of image-guided techniques such as Total Marrow Irradiation (TMI) and Total Marrow and Lymphoid Irradiation (TMLI) via tomotherapy platforms marks a shift toward more tailored and precise conditioning regimens
| [17] | Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279. https://doi.org/10.1016/j.ijrobp.2008.04.071 |
| [19] | V. Sarradin, L. Simon, A. Huynh, et al.: Total body irradiation using Helical Tomotherapy®: Treatment technique, dosimetric results and initial clinical experience. Cancer Radiother. 201822, 17-24. https://doi.org/10.1016/j.canrad.2017.06.014 |
| [20] | S. R. Faught, S. Y. Firat, C. A. Lawton, et al.: A Dosimetric Comparison of Conventional Radiotherapy and Helical Tomotherapy (HT) for Total Body Irradiation (TBI). Int J Radiat Oncol Biol. 200872, https://doi.org/10.1016/j.ijrobp.2008.06.1452 |
[17, 19, 20]
. A comprehensive review has also consolidated the clinical value of TBI in bone marrow transplantation regimens and highlighted emerging trends in advanced radiotherapy modalities
.
Despite the conformal capabilities of VMAT/RapidArc in delivering TBI, these approaches face logistical and dosimetric limitations compared to tomotherapy. VMAT based TBI often necessitates multiple isocenters and arcs due to restricted field lengths, introducing the need for junctions between treatment fields
| [14] | Köksal M., Özkan O., Holderried T, et al.: Optimized conformal total body irradiation with VMAT using a linear-accelerator-based radiosurgery treatment system in comparison to the golden standard helical TomoTherapy. Cancers. 202315. https://doi.org/10.3390/cancers15174220 |
| [15] | Thanvi S, Shinde R, Chandar H, et al.: Dosimetric comparison of VMAT vs 3DCRT in TBI using single HFS CT scan with anterior-posterior/posterior-anterior (AP/PA) field matching in cranial and caudal junctions. Asian Pac J Cancer Care. 2024: 49-53. https://doi.org/10.31557/APJCC.2024.9.1.49-53 |
| [17] | Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279. https://doi.org/10.1016/j.ijrobp.2008.04.071 |
| [22] | Hoeben BAW, Wong JYC, Fog LS, et al.: Total Body Irradiation in Haematopoietic Stem Cell Transplantation for Paediatric Acute Lymphoblastic Leukaemia: Review of the Literature and Future Directions. Front Pediatr. 20219, 774348: https://doi.org/10.3389/fped.2021.774348 |
[14, 15, 17, 22]
. These junctions are susceptible to inaccuracies, potentially leading to hot or cold spots that compromise dose uniformity. Conversely, the continuous delivery offered by tomotherapy eliminates field junctions, resulting in more homogeneous dose coverage
| [17] | Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279. https://doi.org/10.1016/j.ijrobp.2008.04.071 |
| [18] | Susanta K. Hui, Jeff Kapatoes, Jack Fowler, et al.: Feasibility study of helical tomotherapy for total body or total marrow irradiation. Med Phys. 200532, 3214: 3224. https://doi.org/10.1118/1.2044428 |
| [19] | V. Sarradin, L. Simon, A. Huynh, et al.: Total body irradiation using Helical Tomotherapy®: Treatment technique, dosimetric results and initial clinical experience. Cancer Radiother. 201822, 17-24. https://doi.org/10.1016/j.canrad.2017.06.014 |
[17-19]
.
Planning complexity is also greater with VMAT, as it requires precise coordination of isocenters, arc overlaps, and patient repositioning, especially when switching between head-first and feet-first orientations. This can increase both the planning workload and the potential for setup errors
| [14] | Köksal M., Özkan O., Holderried T, et al.: Optimized conformal total body irradiation with VMAT using a linear-accelerator-based radiosurgery treatment system in comparison to the golden standard helical TomoTherapy. Cancers. 202315. https://doi.org/10.3390/cancers15174220 |
| [15] | Thanvi S, Shinde R, Chandar H, et al.: Dosimetric comparison of VMAT vs 3DCRT in TBI using single HFS CT scan with anterior-posterior/posterior-anterior (AP/PA) field matching in cranial and caudal junctions. Asian Pac J Cancer Care. 2024: 49-53. https://doi.org/10.31557/APJCC.2024.9.1.49-53 |
| [17] | Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279. https://doi.org/10.1016/j.ijrobp.2008.04.071 |
| [22] | Hoeben BAW, Wong JYC, Fog LS, et al.: Total Body Irradiation in Haematopoietic Stem Cell Transplantation for Paediatric Acute Lymphoblastic Leukaemia: Review of the Literature and Future Directions. Front Pediatr. 20219, 774348: https://doi.org/10.3389/fped.2021.774348 |
[14, 15, 17, 22]
. In contrast, tomotherapy enables treatment in a single position, enhancing immobilization consistency and setup reproducibility
| [17] | Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279. https://doi.org/10.1016/j.ijrobp.2008.04.071 |
| [18] | Susanta K. Hui, Jeff Kapatoes, Jack Fowler, et al.: Feasibility study of helical tomotherapy for total body or total marrow irradiation. Med Phys. 200532, 3214: 3224. https://doi.org/10.1118/1.2044428 |
[17, 18]
.
Another challenge with VMAT lies in its limited longitudinal field size (typically up to 40 cm), necessitating multiple field splits and dose summation, whereas tomotherapy can treat larger anatomical extents without interruption
| [14] | Köksal M., Özkan O., Holderried T, et al.: Optimized conformal total body irradiation with VMAT using a linear-accelerator-based radiosurgery treatment system in comparison to the golden standard helical TomoTherapy. Cancers. 202315. https://doi.org/10.3390/cancers15174220 |
| [15] | Thanvi S, Shinde R, Chandar H, et al.: Dosimetric comparison of VMAT vs 3DCRT in TBI using single HFS CT scan with anterior-posterior/posterior-anterior (AP/PA) field matching in cranial and caudal junctions. Asian Pac J Cancer Care. 2024: 49-53. https://doi.org/10.31557/APJCC.2024.9.1.49-53 |
| [17] | Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279. https://doi.org/10.1016/j.ijrobp.2008.04.071 |
| [22] | Hoeben BAW, Wong JYC, Fog LS, et al.: Total Body Irradiation in Haematopoietic Stem Cell Transplantation for Paediatric Acute Lymphoblastic Leukaemia: Review of the Literature and Future Directions. Front Pediatr. 20219, 774348: https://doi.org/10.3389/fped.2021.774348 |
[14, 15, 17, 22]
. While VMAT may deliver faster beam on times, overall treatment duration is often prolonged due to repositioning and image verification steps. Tomotherapy offers a more integrated workflow with automated imaging and precise delivery
| [16] | J P Cleuziou, C. Desgranges, I. Henry, et al.: Total body irradiation using helical tomotherapy: Set-up experience and in-vivo dosimetric evaluation. Cancer Radiother. 202125, 213-221. https://doi.org/10.1016/j.canrad.2020.07.009 |
| [18] | Susanta K. Hui, Jeff Kapatoes, Jack Fowler, et al.: Feasibility study of helical tomotherapy for total body or total marrow irradiation. Med Phys. 200532, 3214: 3224. https://doi.org/10.1118/1.2044428 |
| [19] | V. Sarradin, L. Simon, A. Huynh, et al.: Total body irradiation using Helical Tomotherapy®: Treatment technique, dosimetric results and initial clinical experience. Cancer Radiother. 201822, 17-24. https://doi.org/10.1016/j.canrad.2017.06.014 |
| [22] | Hoeben BAW, Wong JYC, Fog LS, et al.: Total Body Irradiation in Haematopoietic Stem Cell Transplantation for Paediatric Acute Lymphoblastic Leukaemia: Review of the Literature and Future Directions. Front Pediatr. 20219, 774348: https://doi.org/10.3389/fped.2021.774348 |
[16, 18, 19, 22]
. Furthermore, the in-built imaging modalities in tomotherapy systems, either MVCT or KVCT, provide superior anatomical visualization and coverage compared to the narrower cone beam CT (CBCT) commonly used with VMAT systems
| [17] | Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279. https://doi.org/10.1016/j.ijrobp.2008.04.071 |
| [19] | V. Sarradin, L. Simon, A. Huynh, et al.: Total body irradiation using Helical Tomotherapy®: Treatment technique, dosimetric results and initial clinical experience. Cancer Radiother. 201822, 17-24. https://doi.org/10.1016/j.canrad.2017.06.014 |
[17, 19]
.
Despite the technological advancements in tomotherapy based Total Body Irradiation (TBI), the practical clinical workflow remains challenging, particularly due to the standard requirement for two separate CT simulations-head-first supine (HFS) for the upper body and feet-first supine (FFS) for the lower body. This dual-position imaging approach introduces several logistical and technical complications. Firstly, it requires the patient to be repositioned midway through the planning CT acquisition, which is both time consuming and physically taxing, especially for pediatric or debilitated patients. During treatment delivery, this dual setup also necessitates interrupting the treatment session to physically move the patient off the couch, reorient them into the FFS position, and reestablish accurate alignment and immobilization, adding complexity and extending the overall treatment time.
To address these challenges, recent methods use single-position imaging with a single HFS CT scan, eliminating the need for FFS repositioning. Additionally, Surface Guided Radiation Therapy (SGRT) systems enable real-time surface tracking, improving setup accuracy and allowing intra-fraction motion monitoring with automatic beam gating to prevent dose errors.
This work aims to evaluate a simplified TBI technique combining single HFS CT imaging and SGRT motion management, comparing it to the traditional dual CT method, while maintaining treatment accuracy and dosimetric quality.
2. Materials and Methods
2.1. Patient Selection
Table 1. Demographic and clinical dose and fractionation of patients treated with Total Body Irradiation.
Patient | Age Yr | Gender | Diagnosis | Dose | No. of Fractions | CT sim |
1 | 44 | Male | Acute Lymphoblastic Leukemia (ALL) | 2Gy | 1 | Single Whole Body HFS |
2 | 45 | male | Refractory multiple Myloma | 2Gy | 1 | Single Whole Body HFS |
3 | 38 | Male | Refractory multiple Myloma | 2Gy | 1 | Single Whole Body HFS |
4 | 45 | Male | Myloid Fibrosis | 6Gy | 3 | Single Whole Body HFS |
5 | 35 | Male | Refractory Hodgkins Lymphoma | 2Gy | 1 | Single Whole Body HFS |
All patients who underwent Total Body Irradiation (TBI) on the Radixact Tomotherapy system between August 2024 and April 2025 at our institution were retrospectively analyzed for this study. These patients were referred to TBI as part of their pre-transplant conditioning regimen. Before initiation of TBI, each patient provided written informed consent for treatment.
Table 1 shows the details of the Patient.
2.2. CT Simulation
Simulation was performed using a PET-CT scanner capable of acquiring a full-body scan in a single session. Each patient was positioned head-first supine (HFS) for the entire scan. Immobilization was achieved using a vacuum cushion bag molded around the patient's body to minimize movement during treatment. Arms were positioned straight alongside the body and enclosed within the vacuum bag to restrict motion further. A five-clamp thermoplastic mask with a standard headrest was applied for head immobilization.
Three tattoo marks were placed at chest level to facilitate treatment planning. Additionally, two radiopaque markers were placed bilaterally at the mid-thigh level to aid in identifying the junction during planning.
The PET-CT scanner was configured to acquire images with a 5 mm slice thickness, covering the entire body from the vertex to the toes in a single HFS orientation. A reference 3D surface was acquired, which was later used for SGRT-based patient setup and monitoring.
Figure 1 shows the immobilization system used for the simulation.
Figure 1. CT simulation patient positioning and immobilization.
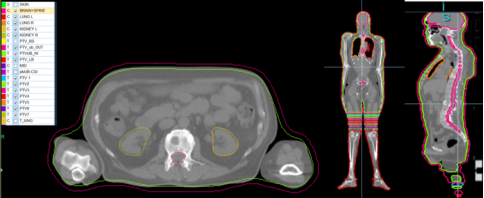
2.3. Contouring and Target Delineation
Accuray Precision (v3.5.0.2) was used for contouring. Target delineation was performed on the simulation CT images. The clinical target volume (CTV) encompassed the patient’s entire external contour. Two planning target volumes (PTVs) were created: PTV_IN, cropped 3 mm beneath the skin surface, and PTV_OUT, extended 5 mm above the skin surface. These PTVs were further divided into upper body, lower body, and seven overlap PTVs.
Critical organs at risk (OARs), including the lungs, kidneys, and lenses of the eyes, were contoured separately for dosimetric documentation. Contouring followed institutional protocols and international guidelines for total body irradiation (TBI) planning.
As shown in
Figure 2, the junction region was identified using mid-thigh markers and carefully divided into seven planning target volumes (PTVs) to facilitate effective dose feathering. These seven PTVs ensured smooth dose transitions at the junction, minimizing hot and cold spots and achieving a more uniform dose distribution across the overlap area.
Figure 2. Clinical contouring for TBI Patients.
2.4. Treatment Planning
All treatment plans were created using the Accuray Precision® v3.5.0.2 planning system, seamlessly integrated with the Radixact® TomoTherapy platform. Plans utilized 6 MV photons and were optimized using VOLO™ Ultra, ensuring precise and effective treatment delivery. For all patients, a consistent field width of 5.0 cm, dynamic jaw mode, and a pitch range of 0.3 to 0.4 were used. These parameters were chosen to provide uniform dose coverage while enhancing treatment efficiency.
The acceleration treatment factor was maintained at the mid-position, resulting in a modulation factor ranging from 1.5 to 2.2. This dynamic adjustment optimized treatment time while minimizing unnecessary radiation exposure. All treatment plans were delivered in helical mode, offering a reproducible and efficient method for Total Body Irradiation (TBI). This approach reduced planning and delivery complexity while maintaining excellent dose homogeneity.
Treatment planning was performed using a single head-first supine (HFS) CT dataset acquired during simulation. From this single dataset, two separate plans were generated:
1) Upper body plan: Covered the region from the head to the mid-thigh.
2) Lower body plan: Covered the region from the mid-thigh to the feet.
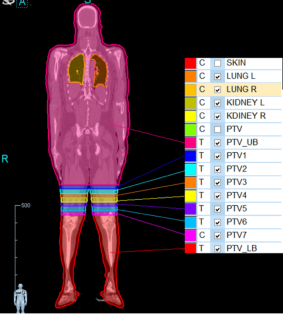
As illustrated in
Figure 3, an intentional overlap region (junction) of approximately 14 cm at the mid-thigh was incorporated between the two plans. This junction was carefully managed by dividing it into seven planning target volumes (PTVs), each 2 cm in the longitudinal direction. Feathering techniques were applied to smooth the dose gradient and minimize inhomogeneity. This strategy ensured a uniform dose distribution across the junction, effectively preventing hot or cold spots.
Figure 3. Target volume segmentation into upper body PTV, lower body PTV, and a feathered overlap region comprising seven sub-PTVs.
Planning Details
1) Plan 1: Upper Body
For the upper body, the optimization goal was to deliver a 2 Gy dose to the PTV Upper Body. A lung constraint was applied with a mean dose (Dmean) limit of 1.7 Gy, to minimize radiation exposure to critical structures. No additional constraints were specified for other organs at risk (OARs) during this phase of treatment.
2) Plan 2: Lower Body
For the lower body, the optimization goal was to deliver a 2 Gy dose to the PTV Lower Body. The dose was prescribed to ensure homogeneity across the lower body.
In the overlap region common to both plans, the prescribed dose was carefully distributed among the seven feathered PTVs. The optimization aimed to achieve dose homogeneity at the junction area, ensuring a smooth transition between the upper and lower body plans while maintaining the 2 Gy prescription dose.
Table 2 shows the distribution of the dose among the seven feathered PTVs in both Plan 1 and Plan 2.
Table 2. Prescribed dose distribution across feathered PTVs in the junction region of upper and lower body plans, expressed as percentages of the prescription dose.
PTV | Upper Body Plan (% of PD) | Lower Body Plan (% of PD) |
PTV 1 | 90% | 10% |
PTV 2 | 80% | 20% |
PTV 3 | 70% | 30% |
PTV 4 | 60% | 40% |
PTV 5 | 50% | 50% |
PTV 6 | 40% | 60% |
PTV 7 | 10% | 90% |
2.5. Plan Evaluation
For the plan evaluation, both the plan summation and dose distribution were thoroughly reviewed. Plan summation was performed in evaluation mode using the treatment planning system (TPS) to combine the upper and lower body plans. This allowed for the assessment of cumulative dose distribution across the entire body, ensuring proper prescription dose at the junction region.
The dose distribution was meticulously examined to identify any potential hot or cold spots, particularly within the junction area. The feathering technique applied in the overlap region was carefully evaluated to ensure there was no significant dose inhomogeneity. Furthermore, Dose Volume Histogram (DVH) data for each PTV and critical organs were analyzed as an objective measure to confirm that all dose constraints were met. Dose homogeneity within the treatment volume was also assessed based on the DVH analysis.
2.6. Treatment Delivery
To ensure accurate patient setup and alignment during Total Body Irradiation (TBI), Surface Guided Radiation Therapy (SGRT) was integrated into both the upper and lower body treatment workflows. SGRT provided non-ionizing, real-time surface tracking, enabling therapists to verify patient positioning based on external surface anatomy before initiating beam delivery.
For the upper body setup, SGRT ensured accurate alignment of the head, chest, and abdomen in the Head-First Supine (HFS) position. This was particularly critical due to the proximity of organs at risk (OARs) such as the lungs and liver. However, one practical challenge during upper body alignment was ensuring that surface contours accurately corresponded to internal anatomy, particularly in the presence of postural changes or irregular breathing. To address this, ClearRT-based kilovoltage CT (KVCT) imaging was employed as a secondary verification tool. It provided high-resolution volumetric images from the vertex to the mid-thigh, including the crucial junction region. This step was essential for detecting any internal misalignments that surface-based tracking alone might miss, especially at the interface between the upper and lower body plans. Following verification, couch corrections were applied as needed, and the upper body treatment was delivered.
For the lower body treatment, instead of repositioning the patient into a Feet-First Supine (FFS) orientation, the workflow utilized longitudinal-only couch shifts, moving the patient upward along with the baseplate. This approach maintained consistent body posture laterally and vertically, preserving alignment while extending treatment coverage to the lower body. The magnitude of this longitudinal shift was determined based on the patient’s height.
SGRT was again employed to verify the alignment of the lower limbs. After rapid surface alignment, ClearRT KVCTimaging was performed from the mid-thigh to the toes to confirm internal anatomy and junction continuity. This dual verification approach, combining SGRT for real-time surface tracking and ClearRT imaging for internal anatomy verification, ensured precise and efficient dosimetric alignment at the junction. It significantly minimized the risk of underdosing or overdosing in this critical transition region.
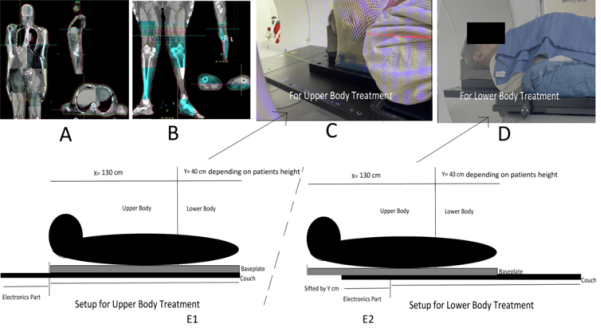
Figure 4 shows the KVCT images for alignment and the position of the baseplate for upper body and lower body treatment.
In both treatments, C-RAD’s SGRT was employed for intra-fraction motion management. During beam delivery, SGRT cameras continuously monitored the patient’s surface in real time to ensure accurate positioning throughout the treatment session. The system was configured to automatically hold the beam if patient movement exceeded predefined tolerance thresholds, thereby enhancing treatment precision and ensuring patient safety by minimizing the risk of geographic miss or unintended radiation exposure to surrounding healthy tissues.
Figure 4. Pre-treatment KVCT imaging and baseplate setup for upper and lower body irradiation (A) Upper body KVCT, (B) lower body KVCT, (C) baseplate positioning on the couch for upper body treatment, (D) longitudinal baseplate displacement for lower body treatment, (E1) schematic diagram of baseplate position during lower body treatment, (E2) baseplate shift during lower body treatment to avoid the feet-first supine position.
2.7. Patient-specific Quality Assurance (QA)
A comprehensive patient-specific quality assurance (PSQA) procedure was performed for each treatment plan to ensure accurate and precise dose delivery. The Delta4 system was used to carry out PSQA measurements for upper and lower body treatment plans. To assess the agreement between planned and delivered doses, gamma analysis was conducted using the 3%/3 mm criteria. This criterion was selected to evaluate the accuracy of the dose distribution and to identify any potential discrepancies between the planned and actual dose delivery.
3. Results
3.1. Imaging and Setup Accuracy
Surface-Guided Radiation Therapy (SGRT) was effectively integrated into the setup verification process for both upper and lower body treatments. For each patient, initial positioning was performed using SGRT to align the patient to the treatment isocenter based on external surface anatomy. This approach enabled rapid, non-invasive, and markerless localization, significantly streamlining the setup workflow.
To validate the accuracy of SGRT-based alignment, kilovoltage computed tomography (kVCT) verification scans were acquired following the initial SGRT setup, covering the vertex to mid-thigh for the upper body plan and thigh to toes for the lower body. These scans served as the reference standard for assessing translational and rotational setup deviations.
As summarized in
Table 3, kVCT verification across five patients demonstrated high geometric accuracy. The mean translational deviations were 0.72 mm (lateral), 1.14 mm (longitudinal), and 1.04 mm (vertical), with 3D vector shifts ranging from 1.54 mm to 1.93 mm (mean: 1.73 mm). Rotational discrepancies were minimal, with average yaw, pitch, and roll values of 0.36°, 0.40°, and 0.24°, respectively. These results confirm the precision and reliability of SGRT in achieving accurate patient alignment for extended-field treatments.
These findings support that SGRT provides high-fidelity initial patient positioning, highly consistent with internal anatomical verification. Its integration into both phases of TBI.
setup-upper and lower body-not only enhances efficiency by reducing reliance on repeated imaging but also ensures accurate, reproducible, and safe patient positioning across extended treatment fields. This reinforces its value in large-field treatments like Total Body Irradiation, where setup reproducibility and patient comfort are critical.
Table 3. Translational and rotational variations from kVCT verification following initial SGRT-based patient setu.
Patient ID | Lateral (mm) | Longitudinal (mm) | Vertical (mm) | 3D Vector Shift (mm) | Yaw (°) | Pitch (°) | Roll (°) |
1 | 0.5 | 1.1 | 1 | 1.57 | 0.4 | 0.5 | 0.3 |
2 | 0.7 | 1.3 | 0.9 | 1.73 | 0.3 | 0.4 | 0.2 |
3 | 0.4 | 1.1 | 1 | 1.54 | 0.6 | 0.5 | 0.4 |
4 | 1.1 | 0.9 | 1.2 | 1.86 | 0.3 | 0.3 | 0.2 |
5 | 0.9 | 1.3 | 1.1 | 1.93 | 0.2 | 0.3 | 0.1 |
The 3D vector shift was calculated as the square root of the sum of the squares of the lateral, longitudinal, and vertical translational deviations.
3.2. Intra-fraction Motion Management with SGRT
During beam delivery, Surface-Guided Radiation Therapy (SGRT) played a critical role in ensuring intra-fractional motion management by providing continuous real-time tracking of the patient’s surface anatomy. The system was configured with clinically appropriate positional and rotational thresholds, enabling it to detect deviations from the planned position with high sensitivity. If patient movement exceeded the predefined tolerance limits, automatic beam-hold functionality was triggered immediately to interrupt radiation delivery.
This feature was particularly vital in junctional regions, where precise dose matching between the upper and lower body plans is essential to avoid underdosing or overdosing due to misalignment. Across the total treatment course for five ptients, more than 90% of all treatment fractions were delivered without interruption, indicating stable and reproducible patient positioning with excellent motion compliance.
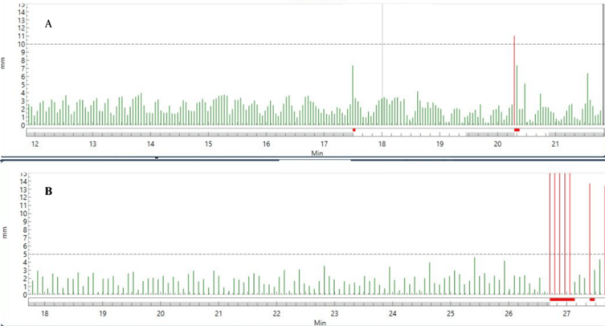
As shown in
Figure 5, in two patients, beam interruptions were recorded during a few instances. These occurrences were primarily associated with deep or irregular breathing patterns during the lower body irradiation phase. The beam-hold mechanism functioned as intended, pausing treatment until the patient returned within the acceptable motion threshold, after which delivery resumed automatically without manual intervention.
Figure 5. Intra-fraction motion management data showing beam holds triggered by sudden patient movements, indicated by red bars. A. Motion monitoring data of one patient and B. is Motion monitoring data of another patient.
Post-treatment, SGRT session logs were exported and analyzed using TQA software to evaluate system responsiveness and beam-hold latency. The average Beam-Off Latency (time between threshold breach and beam interruption) was measured at 0.0038 seconds, confirming the system’s capability for near-instantaneous response, thereby preserving treatment accuracy and patient safety.
These findings reinforce the reliability of SGRT not only for initial setup but also as a robust real-time monitoring solution for extended-field treatments like Total Body Irradiation (TBI), where patient compliance and positional accuracy during longer beam-on times are critical.
3.3. Plan Evaluation and Dosimetry
A comprehensive plan evaluation was conducted for all five patients to ensure adequate target coverage, homogeneity across the full body, including junctional regions.
Each plan, including upper body and lower body segments, was assessed on the single head-first supine (HFS) CT dataset using standard dosimetric parameters. The cumulative dose distribution achieved robust target coverage, with a mean of 95% of the PTV volume receiving at least 95% of the prescribed dose across all patients. The maximum dose to the PTV (Dmax) remained within acceptable clinical limits (< 120% of the prescription dose), ensuring hotspots were well controlled.
Lung mean doses averaged around 170 for a 2 Gy prescription dose and 510 cGy for a 6 Gy prescription. Treatment times for the upper body varied from approximately 1256 to 1600 seconds, and for the lower body from 646 to 835 seconds. Modulation indices ranged from 1.4 to 2.3 for upper and lower body plans, reflecting plan complexity.
The dose homogeneity index (HI) was calculated by the formula defined as
Dmax = Maximum dose in PTV in Gy, Dp = Prescription dose in Gy
HI was calculated for each patient’s cumulative PTV. The homogeneity index (HI) remained between 1.16 and 1.21, indicating uniform dose distribution. Particular attention was paid to the junction region, the overlap between the upper and lower plans. The dose profile across the junction was smooth and continuous, with no significant dose dips or peaks above 123% of the prescribed dose observed.
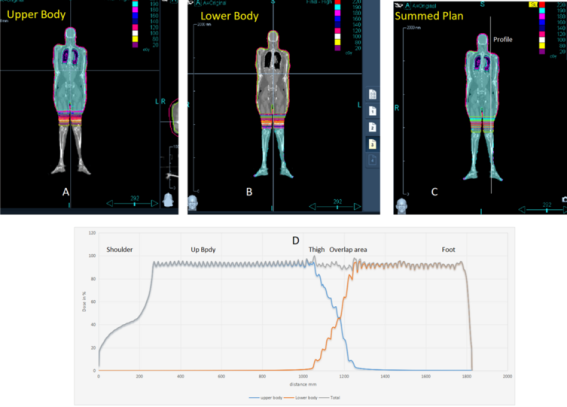
Table 4 summarizes the dose statistics and plan details, and
Figure 6 shows the dose distribution and dose profile at the overlap region.
Figure 6. Dose distributions for upper and lower body plans with cumulative summed dose showing the uniformity at the junction. (A) Dose distribution for upper body plan, (B) dose distribution for lower body plan, (C) Cumulative summed dose distribution, (D) Dose profile across the junction region showing hot and cold spot verification.
Table 4. PTV and OAR Dose Statistics with Treatment Time and Modulation Factor.
| | PTV Dose cGy | | Upper Body | Lower Body |
Patient | Dose/Fr | D95 | D10 | D2 | Dmean | Dmax | PTV HI | Lung Dmean cGy | Treatment Time sec | Modulation Index | Treatment Time sec | Modulation Index |
1 | 2Gy/1fr | 195 | 209 | 212 | 203 | 242 | 1.21 | 173 | 1275.3 | 1.8 | 680 | 1.9 |
2 | 2Gy/1fr | 192.6 | 208.5 | 211 | 200 | 240 | 1.2 | 170 | 1600.3 | 2.1 | 835 | 2.3 |
3 | 2Gy/1fr | 192 | 208 | 211 | 201 | 240 | 1.2 | 175 | 1256 | 1.5 | 646.4 | 1.5 |
4 | 6Gy/3fr | 190 | 620 | 631 | 605 | 707 | 1.18 | 510 | 1297 | 1.4 | 704 | 1.5 |
5 | 2Gy/1fr | 190.6 | 210 | 215 | 203 | 235 | 1.16 | 177 | 1257 | 1.7 | 673 | 1.8 |
3.4. Pretreatment Patient-specific QA
Pretreatment verifications for the five patients were performed using the Delta4 phantom. For each patient, QA measurements were conducted at three anatomical levels: head to thorax, thorax to abdomen, and thigh to toe. The results demonstrated a strong correlation between the planned and delivered doses.
The mean gamma passing rate for the head to thorax region was 97.34%, with individual values ranging from 95.9% to 98.6%. For the thorax to abdomen region, the mean was 96.66%, with a range of 96.2% to 97.9%, and the thigh region exhibited the highest mean passing rate of 98.38%, ranging from 97.9% to 98.7%.
The gamma index analysis using the 3%/3 mm criteria is summarized in
Table 5.
Table 5. Patient-specific QA: Gamma passing rates at different body locations using the 3%/3 mm criterion, measured on the Delta4 patient-specific QA phantom.
Patient ID | Head to Thorax (%) | Thorax to Abdomen (%) | Thigh to Toe (%) |
1 | 98.6 | 97.9 | 98.2 |
2 | 96.1 | 97.4 | 98.6 |
3 | 97.8 | 97.5 | 97.9 |
4 | 98.3 | 97.3 | 98.5 |
5 | 95.9 | 96.2 | 98.7 |
4. Discussion
The conventional approach of acquiring separate CT scans in both head-first supine (HFS) and feet-first supine (FFS) positions adds logistical challenges and introduces opportunities for geometric misalignment, dosimetric uncertainty, and increased planning workload.
Several studies have attempted to optimize TBI delivery through techniques like helical tomotherapy, and volumetric arc delivery, demonstrating the feasibility of helical tomotherapy for TBI with good dose uniformity and lung sparing. However, most of these studies still relied on dual CT datasets and complex image registration for dose summation, which remain sources of inter-plan variability.
One of the most prominent advantages of this simple HFS-only Total Body Irradiation (TBI) approach was the substantial improvement in both clinical workflow efficiency and patient experience.
Traditionally, TBI delivery involves acquiring two separate CT datasets, one in HFS orientation for the upper body and another in FFS orientation for the lower body. This dual-scan method introduces added complexity and increases the time required for simulation, planning, and patient positioning. By eliminating the need for a separate FFS CT acquisition and using a single HFS CT scan for both upper and lower body treatment plans, we observed an average simulation time reduction of 15-20 minutes per patient.
During treatment, a simple longitudinal couch shift was used to reposition the patient for lower body irradiation, avoiding the need to remove and reorient the patient on the couch. This reduced in-room setup time by an additional 10-12 minutes per fraction, simplified logistics, and minimized physical strain on both patient and staff. With the aid of Surface-Guided Radiation Therapy (SGRT), the repositioning was accurate and reproducible without requiring additional radiographic imaging or manual realignment.
Patients reported improved tolerance due to the reduced setup complexity and shorter treatment time; there was a notable increase in comfort and a decrease in anxiety levels, reflecting a more patient-friendly experience overall.
Beyond the physical setup, significant benefits were realized in treatment planning, particularly through the streamlined data flow enabled by using a single CT dataset. This approach eliminated the need to import and manage two separate image sets, simplifying the entire planning process. Contouring was more efficient and consistent, as all organs-at-risk (OARs) and the planning target volume (PTV) could be delineated on a unified dataset. This avoided the need to create separate feathered PTVs on different scans (such as upper and lower CTs), a practice that often introduces variability and geometric uncertainties at the junction. Additionally, no image registration was necessary between the two datasets, bypassing the conventional requirement for deformable image registration (DIR) to align head-first supine (HFS) and feet-first supine (FFS) scans before dose summation, a step that is not only error-prone but also demands rigorous quality assurance. Dose summation itself became simpler and more accurate, as both upper and lower plans could be directly summed on a single CT without deformable fusion, enhancing dosimetric precision, especially in the junction region. Overall, this approach significantly reduced planning time, improved workflow robustness, and minimized opportunities for errors related to data handling, contour propagation, and image fusion.
Surface Guided Radiation Therapy (SGRT) was critical to this workflow. It enabled accurate and reproducible patient setup for both treatment segments. Usually, manual patient positioning requires multiple kVCTs and repositioning, but SGRT enables initial accurate positioning without additional imaging or physical repositioning. Moreover, SGRT provided real-time intrafraction motion monitoring, effectively triggering beam holds during excessive movement, with sub-second latency, ensuring precise dose delivery, especially critical at the junction.
From a dosimetric standpoint, treatment plans achieved excellent target coverage, PTV homogeneity, and smooth dose continuity across the junction region. The use of a single CT dataset also avoided the need for complex image registration, deformable dose summation, and repeated contouring across two datasets, significantly improving workflow efficiency.
One of the limitations of this study is the requirement for a CT scanner capable of full-body scanning. Conventional CT machines or CT simulators may not support scanning the entire body in a single acquisition, which poses a challenge for implementing this approach widely. To overcome this constraint, we utilized a PET-CT scanner for simulation, as it allowed full-body imaging in a head-first supine orientation. However, since the PET-CT differs from the treatment planning CT system, a separate CT-to-electron density (ED) calibration curve had to be generated specifically for this scanner to ensure accurate dose calculations.
5. Conclusions
The implementation of a single-CT, head-first supine TBI technique combined with SGRT-based setup and motion management presents a highly effective, efficient, and patient-friendly alternative to conventional dual-orientation workflows. This method eliminates the need for feet-first supine (FFS) scanning, minimizes planning complexity, improves dosimetric accuracy at junctions, and enhances overall treatment reproducibility and safety. Our initial clinical experience with five patients confirms the feasibility, accuracy, and workflow advantages of this approach.
Abbreviations
DX | Dose Receiving X% of the PTV Volume |
Dmean | Mean Dose |
HI | Homogeneity Index |
Dmax | Maximum Dose |
PTV | Planning Target Volume |
SGRT | Surface Guided Radiotherapy |
DIR | Deformable Image Registration |
KVCT | Kilo Voltage Computed Topography |
Conflicts of Interest
The authors declare no conflicts of interest
References
| [1] |
Gruen A, Ebell W, Wlodarczyk W, et al.: Helical tomotherapy for total body irradiation - a prospective study of dosimetric quality, feasibility, and acute toxicity. Radiat Oncol. 20138, 92-10.
https://doi.org//10.1186/1748-717X-8-92
|
| [2] |
Khan FM, Gibbons JP: The Physics of Radiation Therapy. Philadelphia, PA: Lippincott Williams & Wilkins; 2014.
|
| [3] |
Halperin EC, Constine LS, Tarbell NJ, Kun LE: Pediatric Radiation Oncology. Philadelphia, PA. Lippincott Williams & Wilkins, 2010.
https://link.springer.com/content/pdf/10.1007/978-3-319-43545-9.pdf
|
| [4] |
Heublein AC. A: Preliminary report on continuous irradiation of the entire body. Radiology. 193218, 1051-1062.
https://doi.org/10.1148/18.6.1051
|
| [5] |
Deeg HJ, Sullivan KM, Buckner CD, et al.: Marrow transplantation for acute nonlymphoblastic leukemia in first remission: toxicity and long-term follow-up of patients conditioned with single dose or fractionated total body irradiation. Bone Marrow Transplant. 1986, 1: 151-157.
|
| [6] |
Girinsky T, Benhamou E, Bourhis JH, et al.: Prospective randomized comparison of single-dose versus hyperfractionated total-body irradiation in patients with hematologic malignancies. J Clin Oncol. 200018, 981-986.
https://doi.org/10.1200/JCO.2000.18.5.981
|
| [7] |
Van Dyk J, Galvin J, Glasgow G, Podgorsak E: AAPM Report No. 17. The physical aspects of total and half body photon irradiation. New York: American Association of. Physicists in Medicine. 1986.
|
| [8] |
Chretien M, Cote C, Blais R, et al.: A variable speed translating couch technique for total body irradiation. Med Phys. 200027, 1127-1130.
https://doi.org/10.1118/1.598978
|
| [9] |
Brown DW, Knibutat K, Edmonds N, et al.: A novel translational total body irradiation technique. J Med. 2010031003,
https://doi.org/10.1115/1.4001864
|
| [10] |
Hussain A, Villarreal-Barajas JE, Dunscombe P, Brown DW: Aperture modulated, translating bed total body irradiation. Med Phys. 201138, 932-941.
https://doi.org//10.1118/1.3534196
|
| [11] |
Springer A, Hammer J, Winkler E, et al.: Total body irradiation with volumetric modulated arc therapy: dosimetric data and first clinical experience. Radiat Oncol. 201611, 46.
https://doi.org/10.1186/s13014-016-0625-7
|
| [12] |
Tas B, Durmus IF, Okumus A, et al.: Total-body irradiation using linac-based volumetric modulated arc therapy: Its clinical accuracy, feasibility and reliability. Radiother Oncol. 2018: 527-533.
https://doi.org/10.1016/j.radonc.2018.08.005
|
| [13] |
Ouyang L, Folkerts M, Zhang Y, et al.: Volumetric modulated arc therapy based total body irradiation: Workflow and clinical experience with an indexed rotational immobilization system. Phys Imaging Radiat Oncol. 20174, 22-25.
https://doi.org/10.1016/j.phro.2017.11.002
|
| [14] |
Köksal M., Özkan O., Holderried T, et al.: Optimized conformal total body irradiation with VMAT using a linear-accelerator-based radiosurgery treatment system in comparison to the golden standard helical TomoTherapy. Cancers. 202315.
https://doi.org/10.3390/cancers15174220
|
| [15] |
Thanvi S, Shinde R, Chandar H, et al.: Dosimetric comparison of VMAT vs 3DCRT in TBI using single HFS CT scan with anterior-posterior/posterior-anterior (AP/PA) field matching in cranial and caudal junctions. Asian Pac J Cancer Care. 2024: 49-53.
https://doi.org/10.31557/APJCC.2024.9.1.49-53
|
| [16] |
J P Cleuziou, C. Desgranges, I. Henry, et al.: Total body irradiation using helical tomotherapy: Set-up experience and in-vivo dosimetric evaluation. Cancer Radiother. 202125, 213-221.
https://doi.org/10.1016/j.canrad.2020.07.009
|
| [17] |
Won JYC, Rosenthal J, Liu A, et al.: Image guided total marrow irradiation (TMI) using helical TomoTherapy in patients with multiple myeloma and acute leukemia undergoing hematopoietic cell transplantation (HCT). Int J Radiat Oncol Biol. 200973, 273-279.
https://doi.org/10.1016/j.ijrobp.2008.04.071
|
| [18] |
Susanta K. Hui, Jeff Kapatoes, Jack Fowler, et al.: Feasibility study of helical tomotherapy for total body or total marrow irradiation. Med Phys. 200532, 3214: 3224.
https://doi.org/10.1118/1.2044428
|
| [19] |
V. Sarradin, L. Simon, A. Huynh, et al.: Total body irradiation using Helical Tomotherapy®: Treatment technique, dosimetric results and initial clinical experience. Cancer Radiother. 201822, 17-24.
https://doi.org/10.1016/j.canrad.2017.06.014
|
| [20] |
S. R. Faught, S. Y. Firat, C. A. Lawton, et al.: A Dosimetric Comparison of Conventional Radiotherapy and Helical Tomotherapy (HT) for Total Body Irradiation (TBI). Int J Radiat Oncol Biol. 200872,
https://doi.org/10.1016/j.ijrobp.2008.06.1452
|
| [21] |
Paix A, Antoni D, Waissi W, et al.: Total body irradiation in allogeneic bone marrow transplantation conditioning regimens: A review. Crit Rev Oncol Hematol. 2018123, 138-148.
https://doi.org/10.1016/j.critrevonc.2018.01.011
|
| [22] |
Hoeben BAW, Wong JYC, Fog LS, et al.: Total Body Irradiation in Haematopoietic Stem Cell Transplantation for Paediatric Acute Lymphoblastic Leukaemia: Review of the Literature and Future Directions. Front Pediatr. 20219, 774348:
https://doi.org/10.3389/fped.2021.774348
|
Cite This Article
-
APA Style
Nirhali, A., Naik, V., Pagare, R., Hunugundmath, S., Deputy, M., et al. (2025). No More Feet-first Supine: A Simplified Total Body Irradiation Planning and Delivery Using Single Head-first Supine CT Simulation and SGRT for Intra-fraction Motion Monitoring on Radixact Tomotherapy. International Journal of Clinical Oncology and Cancer Research, 10(3), 110-120. https://doi.org/10.11648/j.ijcocr.20251003.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Nirhali, A.; Naik, V.; Pagare, R.; Hunugundmath, S.; Deputy, M., et al. No More Feet-first Supine: A Simplified Total Body Irradiation Planning and Delivery Using Single Head-first Supine CT Simulation and SGRT for Intra-fraction Motion Monitoring on Radixact Tomotherapy. Int. J. Clin. Oncol. Cancer Res. 2025, 10(3), 110-120. doi: 10.11648/j.ijcocr.20251003.11
Copy
|
Download
AMA Style
Nirhali A, Naik V, Pagare R, Hunugundmath S, Deputy M, et al. No More Feet-first Supine: A Simplified Total Body Irradiation Planning and Delivery Using Single Head-first Supine CT Simulation and SGRT for Intra-fraction Motion Monitoring on Radixact Tomotherapy. Int J Clin Oncol Cancer Res. 2025;10(3):110-120. doi: 10.11648/j.ijcocr.20251003.11
Copy
|
Download
-
@article{10.11648/j.ijcocr.20251003.11,
author = {Amit Nirhali and Vishram Naik and Rupesh Pagare and Sanjay Hunugundmath and Maria Deputy and Sharad Gadhave},
title = {No More Feet-first Supine: A Simplified Total Body Irradiation Planning and Delivery Using Single Head-first Supine CT Simulation and SGRT for Intra-fraction Motion Monitoring on Radixact Tomotherapy
},
journal = {International Journal of Clinical Oncology and Cancer Research},
volume = {10},
number = {3},
pages = {110-120},
doi = {10.11648/j.ijcocr.20251003.11},
url = {https://doi.org/10.11648/j.ijcocr.20251003.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcocr.20251003.11},
abstract = {Introduction: Total Body Irradiation (TBI) remains a crucial preparatory regimen for hematopoietic stem cell transplantation. However, traditional techniques involve complex workflows requiring dual CT simulations-Head-First Supine (HFS) and Feet-First Supine (FFS)-which pose logistical, dosimetric, and patient comfort challenges. This study introduces a simplified TBI approach using a single HFS CT scan combined with Surface Guided Radiation Therapy (SGRT) for setup verification and intra-fraction motion monitoring on the Radixact® TomoTherapy system. Materials and Methods: From August 2024 to April 2025, five adult patients with hematologic malignancies scheduled for TBI were retrospectively analyzed. Each patient underwent a single HFS simulation scan on PET-CT with full-body coverage. Immobilization was achieved using a vacuum cushion and thermoplastic mask. Treatment planning was performed using Accuray Precision® version 3.5.0.2 on a single CT dataset. Two helical plans, one for the upper body and one for the lower body, were generated with a 14 cm overlap at the mid-thigh. Seven feathered Planning Target Volumes (PTVs) were created at the junction to ensure dose homogeneity. Surface Guided Radiation Therapy (SGRT) was used for initial setup and intra-fraction motion monitoring, while ClearRT-based kVCT imaging served as a secondary internal verification. Patient-specific quality assurance (PSQA) was conducted using Delta4 with 3%/3 mm gamma criteria, and junction dose validation was performed using ion chamber measurements. Results: SGRT enabled accurate patient setup for TBI, with mean translational errors ≤2 mm and rotational errors ≤0.6° when compared to kVCT verification. Real-time motion monitoring during treatment enabled automatic beam-holds with an average latency of 0.0038 seconds, ensuring precise delivery. Dosimetric results showed excellent target coverage (≥95% of the PTV receiving ≥95% of the prescribed dose) and homogeneous dose distribution. Smooth dose profiles were observed at plan junctions, and lung doses remained within safe limits (~1.7 Gy). Pre-treatment QA demonstrated high gamma pass rates across all body regions (mean ≥96.6%), confirming treatment accuracy. Discussion: This simple modified workflow utilizing a single HFS CT scan for full-body TBI on Radixact eliminates the need for patient repositioning and FFS imaging, thereby simplifying the planning and delivery process. Integration of SGRT provides non-ionizing, real-time monitoring, enhancing setup precision and intra-fraction control. The feathered PTV junction design effectively mitigated dose inhomogeneities. This method demonstrates not only dosimetric robustness but also improved workflow efficiency and patient comfort.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - No More Feet-first Supine: A Simplified Total Body Irradiation Planning and Delivery Using Single Head-first Supine CT Simulation and SGRT for Intra-fraction Motion Monitoring on Radixact Tomotherapy
AU - Amit Nirhali
AU - Vishram Naik
AU - Rupesh Pagare
AU - Sanjay Hunugundmath
AU - Maria Deputy
AU - Sharad Gadhave
Y1 - 2025/07/04
PY - 2025
N1 - https://doi.org/10.11648/j.ijcocr.20251003.11
DO - 10.11648/j.ijcocr.20251003.11
T2 - International Journal of Clinical Oncology and Cancer Research
JF - International Journal of Clinical Oncology and Cancer Research
JO - International Journal of Clinical Oncology and Cancer Research
SP - 110
EP - 120
PB - Science Publishing Group
SN - 2578-9511
UR - https://doi.org/10.11648/j.ijcocr.20251003.11
AB - Introduction: Total Body Irradiation (TBI) remains a crucial preparatory regimen for hematopoietic stem cell transplantation. However, traditional techniques involve complex workflows requiring dual CT simulations-Head-First Supine (HFS) and Feet-First Supine (FFS)-which pose logistical, dosimetric, and patient comfort challenges. This study introduces a simplified TBI approach using a single HFS CT scan combined with Surface Guided Radiation Therapy (SGRT) for setup verification and intra-fraction motion monitoring on the Radixact® TomoTherapy system. Materials and Methods: From August 2024 to April 2025, five adult patients with hematologic malignancies scheduled for TBI were retrospectively analyzed. Each patient underwent a single HFS simulation scan on PET-CT with full-body coverage. Immobilization was achieved using a vacuum cushion and thermoplastic mask. Treatment planning was performed using Accuray Precision® version 3.5.0.2 on a single CT dataset. Two helical plans, one for the upper body and one for the lower body, were generated with a 14 cm overlap at the mid-thigh. Seven feathered Planning Target Volumes (PTVs) were created at the junction to ensure dose homogeneity. Surface Guided Radiation Therapy (SGRT) was used for initial setup and intra-fraction motion monitoring, while ClearRT-based kVCT imaging served as a secondary internal verification. Patient-specific quality assurance (PSQA) was conducted using Delta4 with 3%/3 mm gamma criteria, and junction dose validation was performed using ion chamber measurements. Results: SGRT enabled accurate patient setup for TBI, with mean translational errors ≤2 mm and rotational errors ≤0.6° when compared to kVCT verification. Real-time motion monitoring during treatment enabled automatic beam-holds with an average latency of 0.0038 seconds, ensuring precise delivery. Dosimetric results showed excellent target coverage (≥95% of the PTV receiving ≥95% of the prescribed dose) and homogeneous dose distribution. Smooth dose profiles were observed at plan junctions, and lung doses remained within safe limits (~1.7 Gy). Pre-treatment QA demonstrated high gamma pass rates across all body regions (mean ≥96.6%), confirming treatment accuracy. Discussion: This simple modified workflow utilizing a single HFS CT scan for full-body TBI on Radixact eliminates the need for patient repositioning and FFS imaging, thereby simplifying the planning and delivery process. Integration of SGRT provides non-ionizing, real-time monitoring, enhancing setup precision and intra-fraction control. The feathered PTV junction design effectively mitigated dose inhomogeneities. This method demonstrates not only dosimetric robustness but also improved workflow efficiency and patient comfort.
VL - 10
IS - 3
ER -
Copy
|
Download