Abstract
Triple-negative breast cancer is a rising concern recently as incidence and deaths have doubled within two years. Despite various proven risk factors and effective therapies, improvements in survival rates have not been up to the mark. This study evaluated 110 patients with histologically proven stage I-III TNBC with invasive ductal carcinoma treated from 2021 to 2023, all of whom underwent surgery, chemotherapy, and radiotherapy. The majority of patients were over 35 years old (69.1%, median age 40±10.6 years), with left-sided cancers being more common (60%), and mastectomy was the primary surgical approach (76.4%), often followed by adjuvant chemotherapy (88%). The most prevalent tumor size was T2 (88.2%) and nodal status was N1 (52.7%), with T2 and N1 showing significant prevalence across surgical and chemotherapy groups; recurrence was higher in patients receiving neoadjuvant chemotherapy and lumpectomy, while survival was higher with mastectomy compared to lumpectomy and with adjuvant versus neoadjuvant chemotherapy. The findings suggest that adjuvant chemotherapy and mastectomy with radiotherapy have a significant effect on the 2-year survival of TNBC patients in this cohort, reinforcing the prognostic importance of tumor stage and nodal involvement. This may have a vital role in the prognosis of the disease and has a huge scope for research.
Keywords
Breast Cancer, TNBC, Mastectomy, Lumpectomy, Adjuvant Chemotherapy. Neo-adjuvant Chemotherapy, Survival
1. Introduction
Breast cancer (BC) is the most prevalent cancer diagnosed annually in the world and the leading cause of cancer-related deaths among females. According to GLOBOCAN 2022 data, the incidence and mortality of breast cancer were reported to be 46.8% and 12.7% respectively.
| [1] | Mubarik S, Yu Y, Wang F, Malik SS, Liu X, Fawad M, Shi F, Yu C. Epidemiological and sociodemographic transitions of female breast cancer incidence, death, case fatality and DALYs in 21 world regions and globally, from 1990 to 2017: An Age-Period-Cohort Analysis. Journal of Advanced Research. 2022 Mar 1; 37: 185-96. https://doi.org/10.1016/j.jare.2021.07.012 |
| [2] | Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2024). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. accessed [06 October 2024]. https://doi.org/10.1007/s00345-024-04949-8 |
[1, 2]
Apart from the hiking cases and deaths, a noticeably higher incidence of breast cancer exists in developed countries; globally where its age-standardized incidence rate was 114.4 and 63.8 per 100,000 among the female population in countries with high or very high and low to medium Human Development Index (HDI) respectively.
| [3] | Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021 Feb 4. Epub ahead of print. PMID: 33538338. https://doi.org/10.3322/caac.21660 |
[3]
Since breast cancer is highly preventable, as proven by various epidemiological studies, more combined steps should be taken as primary or secondary preventive measures. Some of the prominent risk factors include: obesity, physical inactivity, high-protein diet, alcohol consumption and use of contraceptives.
| [4] | Sun YS, Zhao Z, Yang ZN, Xu F, Lu HJ, Zhu ZY, Shi W, Jiang J, Yao PP, Zhu HP. Risk factors and preventions of breast cancer. International journal of biological sciences. 2017 Nov 1; 13(11): 1387. https://doi.org/10.7150/ijbs.21635 |
| [5] | Huang J, Chan PS, Lok V, Chen X, Ding H, Jin Y, Yuan J, Lao XQ, Zheng ZJ, Wong MC. Global incidence and mortality of breast cancer: a trend analysis. Aging (Albany NY). 2021 Feb 2; 13(4): 5748. https://doi.org/10.18632/aging.202502 |
[4, 5]
There are several signs of breast cancer in its early stages, including a lump or thickened tissue in either breast, fluid discharge from the nipples, and a lump or swelling in either armpit. Additionally, changes in the appearance or texture of the skin, such as a rash or redness, crusting, scaly or itchy skin, or redness on or around the nipple, are also significant clinical features.
While ultrasound and mammogram may be used for preliminary screening, biopsy and immunohistochemistry (IHC) remain the only confirmatory methods for diagnosis. Depending on the disease type, stage and progression of cancer, BC is treated with chemotherapy, surgery, radiotherapy and immunotherapy. Mastectomy or breast-conserving surgery is the most common surgical method, especially in operable stage.
| [7] | Forrai G, Kovács E, Ambrózay É, Barta M, Borbély K, Lengyel Z, Ormándi K, Péntek Z, Tünde T, Sebő É. Use of diagnostic imaging modalities in modern screening, diagnostics and management of breast tumours 1st central-eastern European professional consensus statement on breast cancer. Pathology and Oncology Research. 2022 Jun 8; 28: 1610382. https://doi.org/10.3389/pore.2022.1610382 |
| [8] | Tasmuth T, Von Smitten K, Hietanen P, Kataja M, Kalso E. Pain and other symptoms after different treatment modalities of breast cancer. Annals of oncology. 1995 May 1; 6(5): 453-9. https://doi.org/10.1093/oxfordjournals.annonc.a059215 |
[7, 8]
Breast cancer can be subclassified into different subtypes on the basis immunohistochemical (IHC) protein overexpression of estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor type 2 (HER 2) as luminal A (ER-positive; HER 2-negative), luminal B (ER-positive; HER 2-positive); HER 2 enriched (ER-negative; HER 2-positive) and triple-negative or basal-like (ER-negative; HER 2-negative).
Triple-negative breast cancers (TNBC) comprise 15% of all BCs. TNBC is the most fatal among all breast cancers with poor long-term outcomes.
They are considered the most malignant subtype as they are associated with increased tumor size, increased incidence of axillary lymph node involvement and poor prognosis as compared to other subtypes.
Although the incidence and mortality of TNBC are declining, a sharp rise in younger patients is alarming. Several lifestyle factors may have contributed to this rise including increased physical inactivity, dietary consumption of high animal fat, and excess body weight among younger women.
| [11] | Taha Z, Eltom SE. The role of diet and lifestyle in women with breast cancer: an update review of related research in the Middle East. BioResearch open access. 2018 May 1; 7(1): 73-80. https://doi.org/10.1089/biores.2018.0004 |
[11]
Due to the scarcity of drug-targetable receptors for TNBC, there is a dire need for new curative strategies to be discovered. In addition, routine tests of genetic profiling like BRCA 1 & 2 play a crucial role in TNBC’s diagnosis, followed by treatment. The usual use of neo-adjuvant anthracycline/taxane combinations in TNBC is currently being supplemented by immune checkpoint inhibitors, poly(ADP-ribose) polymerase inhibitors, platinum agents, phosphatidylinositol-3-kinase pathway inhibitors and androgen receptor inhibitors.
Especially, TNBC tumors with BRCA1 mutations have seen increased use of DNA-damaging agents such as platinums, as well as of potentiators of DNA damage such as the investigational agent Iniparib and inhibitors of poly-ADP ribose polymerase such as Olaparib. Tyrosine kinase receptor inhibitors and microtubule-targeting inhibitors of cell cycling are also under active investigation. The use of neo-adjuvant treatment with pCR (no residual invasive cancer in the breast and axillary nodes) as a surrogate of overall survival will allow the rapid evaluation and comparison of current and innovative treatments for TNBC.
A fatal disease like TNBC requires numerous in-depth studies in order to establish new and reliable methods of cure. Additionally, the effectiveness of current therapies and surgical procedures in the prognosis of the disease must be evaluated through rigorous clinical research. Although similar studies have been conducted elsewhere, few have been conducted in the South-Asian region, especially Bangladesh. Our aim was to evaluate the effect of chemotherapy (adjuvant or neo-adjuvant) and surgery (lumpectomy or mastectomy) with adjuvant radiotherapy on the survival and recurrence of TNBC patients after 2 years of follow-up. Hence, the findings of this study will not only provide key insights to prescribers but also play a vital role in the treatment of breast cancer.
2. Methods
This prospective follow-up study was conducted at the Department of Clinical Oncology, Bangabandhu Sheikh Mujib Medical University (BSMMU) from January 2021 to December 2023. The initial population of this study was 120 patients of histologically proven TNBC of invasive duct cell carcinoma subtype who underwent treatment in the department, which eventually reduced to 110 patients. Patients receiving treatment between January 2021 and December 2021 were included in the study, and their corresponding status was followed up from January 2023 to December 2023.
All the patients were purposively sampled & received either adjuvant AC-T (Doxorubicin/Adriamycin, Cyclophosphamide followed by Paclitaxel) or neo-adjuvant TAC (Taxotere, Adriamycin and Cyclophosphamide) chemotherapy and underwent some form of surgery as treatment. All patients had received hypo-fractionated radiotherapy (RT) with a total dose of 40.05 GY in 15 fractions and patients undergoing BCS received an additional 5 fractions electron boost radiotherapy to the surgical bed. Written informed consent was obtained from all study participants prior to their participation.
All the necessary information for the study was collected through a semi-structured questionnaire. Patient details, demographic information and personal history like age, tumor location and exposure to risk factors were collected through face-to-face interviews while data on the disease, treatment, surgical procedure and follow-up were taken from medical records. The clinicopathological characteristics of the triple-negative breast cancer patients, including molecular subtyping, histopathological type, grade, stage of the disease, were also obtained from the patient’s medical records. Sampling technique used in this study was purposive sampling. Information on the response was collected after the chemotherapy and radiotherapy was given. For all the socio-demographic and clinical characteristics, frequency analysis was performed as a descriptive analysis method. All continuous data were expressed as mean ± standard deviation (SD). After the data were collected initially, it was compiled and edited accordingly in MS Excel 2016 then carefully analyzed by IBM SPSS (Statistical Package for Social Sciences) version 26.
2.1. Inclusion Criteria
1. Patients aged from 18 years up to 70 years were included
2. Patients with histologically diagnosed triple-negative breast cancer were included
3. Patients diagnosed with invasive ductal carcinoma of the breast
4. Lymph node-positive patients were included
2.2. Exclusion Criteria
1. Patients with metastatic triple negative breast cancer
2. Pregnant women were not considered
3. Patients with co-morbid conditions like chronic bronchitis/ asthma, COPD, coronary heart disease and stroke were excluded
4. Critically ill patients or those suffering from chronic conditions such as CKD, liver cirrhosis or CHF were not included
3. Results
For the purpose of this study, initially 120 patients were enrolled however, 7 people dropped out willingly and 3 were excluded due to lack of follow-up. Hence, the final population consisted of 110 patients with triple-negative breast cancer with invasive duct cell carcinoma who had followed up till the end of the study.
3.1. Demographic Information
Table 1. Distribution of socio-demographic characteristics of the triple-negative breast cancer patients (N=110).
| Frequency (n) | Percentage (%) |
Age (years) | | |
Median | | 40±10.6 |
<35 | 34 | 30.9 |
>35 | 76 | 69.1 |
Minimum | | 25 |
Maximum | | 74 |
Residence | | |
Rural | 46 | 41.8 |
Urban | 64 | 58.2 |
Table 1 states the socio-demographic characteristics of the patients in the study. The majority of the patients 69.1% (n=76) were above 35 years old, whereas only a minor proportion 30.9% (n=34) were below 35 years old. The median age found was 40±10.6 years and the minimum and maximum ages were 25 and 74 respectively. Demographic location of the participants demonstrated that 58.2% (n=64) belonged to urban area on the contrary, 41.8% (n=46) were from rural places.
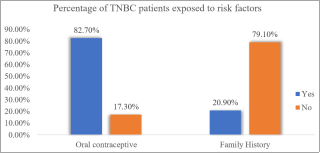
Figure 1. Proportion of triple negative breast cancer patients with exposure to risk factors (N=110).
Figure 1 illustrates the presence of family history and oral contraceptives among the TNBC patients of the study. Oral contraceptive was a prevalent risk factor among 82.7% (n=91) patients, while family history was not a significant risk factor among 20.9% (n=23) patients.
3.2. Clinicopathological Characteristics
Table 2. Distribution of clinicopathological characteristics of the triple-negative breast cancer patients (N=110).
Laterality | Frequency (n) | Percentage (%) |
Left | 65 | 60 |
Right | 45 | 40 |
T-stage | | |
T1 | 5 | 4.5 |
T2 | 97 | 88.2 |
T3 | 3 | 2.7 |
T4 | 5 | 4.5 |
N-status | | |
N0 | 28 | 25.5 |
N1 | 58 | 52.7 |
N2 | 14 | 12.7 |
N3 | 10 | 9.1 |
Table 2 elaborates the various clinicopathological features of the TNBC patients of this study, like laterality, tumor size and nodal status. It was noted that left side dominated with 60% (n=65), however right side was only 40% (n=45). Among tumor stages maximum patients belonged to T2 followed by T1, T4 and T3 consisting of 97 (88.2%), 5 (4.5%), 5 (4.5%) and 3 (2.7%) patients respectively. Almost half of the patients had N1 nodal status bearing 58 (52.7%) patients, the other half had N0 28 (25.5%), N2 14 (12.7%), N3 10 (9.1%) patients.
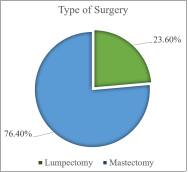
Figure 2. Distribution of patients according to type of surgery (N=110).
Figure 2 shows a pie chart demonstrating the proportion of patients undergoing the two different types of surgery commonly used in the treatment of triple-negative breast cancer. It was observed that majority of patients underwent mastectomy with 84 (76.4%) patients on the contrary, only 26 (23.6%) patients did lumpectomy or breast-conserving surgery either before or after chemotherapy.
Table 3. Distribution of patients by TNM stage (N=110).
TNM Stage | Frequency (n) | Percentage (%) |
Stage I | 4 | 3.6 |
Stage IIA | 26 | 23.6 |
Stage IIB | 46 | 41.8 |
Stage IIIA | 26 | 23.6 |
Stage IIB | 4 | 3.6 |
Stage IIIC | 4 | 3.6 |
Table 3 describes the number and percentages of patients according to TNM staging. Stage IIB revealed the highest percentage having 46 (41.8%), proceeded by stage IIA, IIIA, I, IIB and IIIC with 26 (23.6%), 26 (23.6%), 4 (3.6%), 4 (3.6%) and 4 (3.6%) respectively.
3.3. Intervention and Follow-up
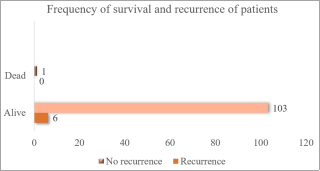
Figure 3. Proportion of triple negative breast cancer patients based on follow-up (N=110).
Figure 3 illustrates a bar chart of the number of patients who survived and recurred the disease. 99.1% (n=109) patients had survived and just 0.9% (n=1) had expired during the study. In addition, only 5.5% (n=6) of patients had recurred the disease.
Table 4. Distribution of TNBC patients and their survival based on type of surgery (N=110).
| Mastectomy (N=84) | Lumpectomy (N=26)a |
T-stage | (84) | (25) |
T1 | 4 (4.8%) | 1 (4%) |
T2 | 75 (89.2%) | 21 (88%) |
T3 | 3 (3.6%) | 0 |
T4 | 2 (2.4%) | 3 (12%) |
Nodal status | (84) | (25) |
N0 | 21 (25%) | 7 (28%) |
N1 | 48 (57.1%) | 9 (36%) |
N2 | 8 (9.5%) | 6 (24%) |
N3 | 7 (8.3%) | 3 (12%) |
Recurrence | 5 (6%) | 1 (3.8%) |
Survival | 84 (100%) | 25 (96.1%) |
Table 4 elaborates the clinical features and subsequent follow-up of triple negative breast cancer patients based on mastectomy or BCS. A total of 84 patients did mastectomy and 26 did lumpectomy or BCS. Among those with mastectomy, 4 (4.8%), 75 (89.2%), 3 (3.6%) and 2 (2.4%) patients had tumor stage T1, T2, T3 and T4 while 21 (25%), 48 (57.1%), 8 (9.5%) and 7 (8.3%) had N0, N1, N2 and N3. Within patients undergoing lumpectomy, 1 (4%), 21 (88%), 0 & 3 (12%) patients expressed T1, T2. T3 & T4 however 7 (28%), 9 (36%), 6 (24%) & 3 (12%) patients had N0, N1, N2 & N3 nodule status.
On the contrary, the disease had recurred in 5 (6%) patients in mastectomy compared to 1 (3.8%) in lumpectomy and survival was 96.1% in lumpectomy versus 100% in mastectomy.
Table 5. Distribution of TNBC patients based on type of chemotherapy (N=110).
| Adjuvant chemotherapy CT= AC-T (N=97) | Neo-adjuvant chemotherapy CT=TAC (N=13)a |
Age (years) | (97) | (12) |
<35 | 29 (29.9%) | 5 (41.6%) |
>35a | 68 (70.1%) | 7 (58.3%) |
T stage | | |
T1 | 4 (4.1%) | 1 (8.3%) |
T2a | 87 (89.7%) | 9 (75%) |
T3 | 3 (3.1%) | 0 |
T4 | 3 (3.1%) | 2 (16.7%) |
Nodal status | (97) | (12) |
N0 | 25 (25.8%) | 3 (25%) |
N1a | 52 (53.6%) | 5 (41.7) |
N2 | 11 (11.3%) | 3 (25%) |
N3 | 9 (9.3%) | 1 (8.3) |
Surgery | (97) | (12) |
Mastectomya | 78 (80.4%) | 5 (41.7%) |
Lumpectomy | 19 (19.6%) | 7 (58.3%) |
Recurrence | 4 (4.1%) | 2 (15.4%) |
Survival | 97 (100%) | 12 (92.3%) |
Table 5 elaborates the presence of clinicopathological features of TNBC patients obtained on the basis of adjuvant or neoadjuvant chemotherapy given. A total of 97 (88.2%) patients had received adjuvant chemotherapy and 13 (11.8%) patients got neo-adjuvant chemotherapy. Out of the patients receiving adjuvant and neo-adjuvant chemotherapy, 29 (29.9%) and 68 (70.1%) were younger than 35 and older than 35 respectively. Adjuvant & Neo-adjuvant patients had majority T2 (89.7%) & (75%) followed by T1, T3 & T4 moreover, their nodal status was N1 (53.6%) & (41.7%) and N0, N2 & N3 remaining 48% & 25%. Although mastectomy topped in the adjuvant chemotherapy group, lumpectomy was higher in the neo-adjuvant group. Recurrence and survival were both lower in neo-adjuvant chemotherapy 2 and 12, compared to adjuvant chemotherapy 4 and 97.
4. Discussion
This prospective follow-up study was conducted to observe the effect of surgery and chemotherapy on the survival of triple-negative breast cancer patients. A total of 110 confirmed patients of invasive duct cell carcinoma of TNBC were assessed based on their surgery and chemotherapy type on survival for 2 years. Out of the patient pool, some of them received adjuvant while others received neo-adjuvant chemotherapy and simultaneously, patients underwent either mastectomy or lumpectomy. The clinicopathological features of the participants were also analyzed and their prevalence was observed. Lastly, the current status of the patients was checked after 2 years of treatment to draw a conclusion.
In our study, we found that a major fraction 69.1% of patients were aged over 35 years old whereas only a minor proportion 30.9% of patients were under 35 years old. Moreover, the median age observed was 40±10.6 years in addition, the minimum and maximum ages were 25 and 74 years respectively. The geographical position of the patients revealed that 58.2% resided in urban areas on the contrary, 41.8% were from rural places. In a similar study, the mean age of 70 patients with TNBC and invasive ductal carcinoma was 49.6 years ±12.6 while the range of age was 27-82 years, in which 20% of patients were below 35 years and 80% above 35 years in age.
| [13] | Payandeh M, Sadeghi M, Sadeghi E, Aeinfar M. Clinicopathology figures and long-term effects of tamoxifen plus radiation on survival of women with invasive ductal carcinoma and triple negative breast cancer. Asian Pacific Journal of Cancer Prevention. 2015; 16(12): 4863-7. https://doi.org/10.7314/APJCP.2015.16.12.4863 |
[13]
Another relevant study assessing 111 patients of TNBC stated the mean age at diagnosis was 63±7 years with an age range of 28-81 years.
| [14] | Bayoumi Y, AbdelSamie A, Abdelsaid A, Radwan A. Locoregional recurrence of triple-negative breast cancer: effect of type of surgery and adjuvant postoperative radiotherapy. Breast Cancer: Targets and Therapy. 2014 Sep 10: 151-8. https://doi.org/10.2147/BCTT.S69309 |
[14]
As per our study, oral contraceptive was seen as a prevalent risk factor among 82.7% of patients, while family history was not a significant risk factor among 20.9% of patients. This implies that the widespread use of contraceptives may have caused a spike in breast cancer patients both globally and countrywide. Oral contraceptive is a modifiable risk factor for breast cancer as reported by Yuniastini et al. (2022).
| [15] | Yuniastini Y, Murhan A, Purwati P, Pratiwi MD. Risk factors for breast cancer: hormonal contraception. Jurnal Aisyah: Jurnal Ilmu Kesehatan. 2022 Jul 25; 7(S1): 349-54. https://doi.org/10.30604/jika.v7iS1.1307 |
[15]
The results of our research showed mastectomy was more common (76.4%) among the patients than lumpectomy (23.6%) either before or after chemotherapy. On the contrary, these results contradict a study that quoted 78.5% of patients had undergone lumpectomy versus 21.5% undergoing mastectomy. It was noted that left-sided tumors dominated with 60% however, a previous study had found that the majority presented with right-sided cancers (53.3%).
| [16] | Wen S, Manuel L, Doolan M, Westhuyzen J, Shakespeare TP, Aherne NJ. Effect of clinical and treatment factors on survival outcomes of triple negative breast cancer patients. Breast Cancer: Targets and Therapy. 2020 Mar 6: 27-35. https://doi.org/10.2147/BCTT.S236483 |
[16]
Among the patients, stage IIB revealed the highest percentage consisting 41.8%, proceeded by stage IIA, IIIA, I, IIB and IIIC with 23.6% 23.6%, 3.6%, 3.6% and 3.6% respectively. This is backed by a similar study where stage II was most common among TNBC patients.
| [13] | Payandeh M, Sadeghi M, Sadeghi E, Aeinfar M. Clinicopathology figures and long-term effects of tamoxifen plus radiation on survival of women with invasive ductal carcinoma and triple negative breast cancer. Asian Pacific Journal of Cancer Prevention. 2015; 16(12): 4863-7. https://doi.org/10.7314/APJCP.2015.16.12.4863 |
| [14] | Bayoumi Y, AbdelSamie A, Abdelsaid A, Radwan A. Locoregional recurrence of triple-negative breast cancer: effect of type of surgery and adjuvant postoperative radiotherapy. Breast Cancer: Targets and Therapy. 2014 Sep 10: 151-8. https://doi.org/10.2147/BCTT.S69309 |
[13, 14]
Considering tumor stages, the maximum number of patients belonged to T2 followed by T1, T4 and T3 consisting of 88.2%, 4.5%, 4.5% and 2.7% patients in this study. Almost half of the patients had N1 nodal status bearing 52.7% patients, the other half had N0 (25.5%), N2 (12.7%) & N3 (9.1%) patients. One of the previous research studies quoted that most patients were T-stage T1 (51.9%), followed by T2 (39.2%) and T3 (6.1%) additionally, the majority were lymph node-negative N0 (62.1%), followed by N1 (22.0%) and N2 (9.3%).
| [16] | Wen S, Manuel L, Doolan M, Westhuyzen J, Shakespeare TP, Aherne NJ. Effect of clinical and treatment factors on survival outcomes of triple negative breast cancer patients. Breast Cancer: Targets and Therapy. 2020 Mar 6: 27-35. https://doi.org/10.2147/BCTT.S236483 |
[16]
Out of the 110 patients, 84 patients had mastectomy and 26 did lumpectomy or BCS surgery. Most of the subjects had T2 tumor stage in both the groups, among those with mastectomy, half of them revealed N1 nodal status while less than half had N1 status in lumpectomy. Within the patients undergoing mastectomy, 4.8%, 89.2%, 3.6% and 2.4% patients had tumor stage T1, T2, T3 and T4 while 25%, 57.1%, 9.5% and 8.3% had N0, N1, N2 and N3. Within the BCS group, 3.9%, 88%, 0 & 11.5% of patients expressed T1, T2. T3 & T4 however, 26.9%, 40%, 23.1% and 11.5% patients had N0, N1, N2 and N3 nodule status. These results reflect similarities with a study stating T3 and T4 tumors and N1, N2 and N3 were more common in the mastectomy group.
| [16] | Wen S, Manuel L, Doolan M, Westhuyzen J, Shakespeare TP, Aherne NJ. Effect of clinical and treatment factors on survival outcomes of triple negative breast cancer patients. Breast Cancer: Targets and Therapy. 2020 Mar 6: 27-35. https://doi.org/10.2147/BCTT.S236483 |
[16]
When assessing the type of chemotherapy, 88.2% of patients had received adjuvant chemotherapy whereas 11.8% of patients had received neo-adjuvant chemotherapy. Out of the patients receiving chemotherapy 29.9% and 70.1% were younger than 35 and older than 35 respectively.
On the contrary, the disease had recurred in 5 patients in mastectomy compared to 1 in lumpectomy and survival was 96.1% in lumpectomy versus 100% in mastectomy. Furthermore, 4 patients recurred in adjuvant chemotherapy and 1 in the neo-adjuvant group with survival of 100% and 92.3%. Overall, it is evident that 99.1% of patients had survived and just 0.9% had expired during the study. Furthermore, only 5.5% of patients had recurred the disease. It can be inferred that adjuvant chemotherapy and mastectomy have a significant effect on the 2-year survival of IDCC TNBC patients apart from tumor stage and nodule involvement which are already scientifically established. This is contrary to Wen S. et al. (2020) where mastectomy was associated with poor survival.
| [16] | Wen S, Manuel L, Doolan M, Westhuyzen J, Shakespeare TP, Aherne NJ. Effect of clinical and treatment factors on survival outcomes of triple negative breast cancer patients. Breast Cancer: Targets and Therapy. 2020 Mar 6: 27-35. https://doi.org/10.2147/BCTT.S236483 |
[16]
Marked improvement was also seen in survival, prognosis and recurrence amongst mastectomy and adjuvant chemotherapy groups of TNBC patients in Bangladesh compared to other countries and their respective outcome was also better. Together, these factors play a key role in the prognosis of the disease and corresponding survival.
5. Limitation and Recommendation
This study acknowledges several limitations that may influence the interpretation and generalizability of its findings. Firstly, the relatively small sample size of 110 patients may limit the statistical power to detect subtle but potentially significant differences, particularly when comparing subgroups within the cohort. Hence, the lack of statistical data makes it challenging to ascertain the statistical significance of the observed results and draw definitive conclusions. Secondly, the study considering a single institution within Bangladesh not only restricts its geographical scope but also affects its acceptability to other populations or healthcare systems. Furthermore, the 2-year follow-up period is relatively short for such research and may not fully capture the long-term outcomes associated with the disease.
In order to prove a possible relationship between the treatment module and survival of TNBC patients, further long-term studies on 5-year and 10-year survival must be done on a broader scale simultaneously possible role of gene mutation should be investigated. Future prospective studies with larger, more diverse cohorts and comprehensive molecular analyses are needed to validate and expand our results. Long-term follow-up of these patients may provide key insights on this topic and further detailed studies are required for drawing a valid conclusion. Several such studies will determine the future course of treatment and hence, have a social impact on the society while improving quality of life of such chronic patients.
6. Conclusion
Triple-negative breast cancer is the most aggressive with an alarming rate of mortality. Nowadays, an increased incidence of TNBC along with poorer prognosis among younger women has raised concerns globally. The effect of oral contraceptive use, tumor stage and nodule involvement is evident from our results and previous studies. Possible benefits of mastectomy and adjuvant chemotherapy may exist in the treatment protocol which should be investigated. Proper treatment design, accurate staging and time of treatment may improve the overall response of the patient. However, there is immense scope for research in finding the causes of the increased incidence and mortality.
Abbreviations
ACT | Adjuvant Chemotherapy (AC-T) |
AC-T | Doxorubicin, Cyclophosphamide Followed by Paclitaxel |
BC | Breast Cancer |
BCS | Breast Conserving Surgery |
BDRT | Boost Dose Radiotherapy |
BRCA | Breast Cancer Gene |
BSMMU | Bangabandhu Sheikh Mujib Medical University |
IDCC | Invasive Duct Cell Carcinoma |
IHC | Immunohistochemical/Immunohistochemistry |
NACT | Neo Adjuvant Chemotherapy (TAC) |
pCR | Pathologic Complete Response |
TAC | Taxotere, Adriamycin & Cyclophosphamide |
TNBC | Triple Negative Breast Cancer |
RT | Radiotherapy |
Author Contributions
Shamsun Nahar: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft
Afsana Sharmin Anika: Data curation, Investigation, Methodology, Project administration, Visualization, Writing – review & editing
Rumana Afroz Majumder: Formal Analysis, Methodology, Project administration, Visualization
Khursheda Akhter: Conceptualization, Methodology, Project administration, Supervision, Writing – original draft
Faruk Ahmed: Conceptualization, Methodology, Project administration, Validation, Writing – original draft
Nasrin Akhter: Data curation, Investigation, Software, Supervision, Writing – review & editing
Fariha Chowdhury: Data curation, Formal Analysis, Methodology, Software, Visualization, Writing – original draft
Saimum Islam: Data curation, Investigation, Resources, Software, Writing – review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Mubarik S, Yu Y, Wang F, Malik SS, Liu X, Fawad M, Shi F, Yu C. Epidemiological and sociodemographic transitions of female breast cancer incidence, death, case fatality and DALYs in 21 world regions and globally, from 1990 to 2017: An Age-Period-Cohort Analysis. Journal of Advanced Research. 2022 Mar 1; 37: 185-96.
https://doi.org/10.1016/j.jare.2021.07.012
|
| [2] |
Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2024). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. accessed [06 October 2024].
https://doi.org/10.1007/s00345-024-04949-8
|
| [3] |
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021 Feb 4. Epub ahead of print. PMID: 33538338.
https://doi.org/10.3322/caac.21660
|
| [4] |
Sun YS, Zhao Z, Yang ZN, Xu F, Lu HJ, Zhu ZY, Shi W, Jiang J, Yao PP, Zhu HP. Risk factors and preventions of breast cancer. International journal of biological sciences. 2017 Nov 1; 13(11): 1387.
https://doi.org/10.7150/ijbs.21635
|
| [5] |
Huang J, Chan PS, Lok V, Chen X, Ding H, Jin Y, Yuan J, Lao XQ, Zheng ZJ, Wong MC. Global incidence and mortality of breast cancer: a trend analysis. Aging (Albany NY). 2021 Feb 2; 13(4): 5748.
https://doi.org/10.18632/aging.202502
|
| [6] |
Crisan D, Crisan M. Dermatologic Concepts and Terminology. Textbook of Dermatologic Ultrasound 2022 Dec 14 (pp. 21-72). Cham: Springer International Publishing.
https://doi.org/10.1007/978-3-031-08736-3_3
|
| [7] |
Forrai G, Kovács E, Ambrózay É, Barta M, Borbély K, Lengyel Z, Ormándi K, Péntek Z, Tünde T, Sebő É. Use of diagnostic imaging modalities in modern screening, diagnostics and management of breast tumours 1st central-eastern European professional consensus statement on breast cancer. Pathology and Oncology Research. 2022 Jun 8; 28: 1610382.
https://doi.org/10.3389/pore.2022.1610382
|
| [8] |
Tasmuth T, Von Smitten K, Hietanen P, Kataja M, Kalso E. Pain and other symptoms after different treatment modalities of breast cancer. Annals of oncology. 1995 May 1; 6(5): 453-9.
https://doi.org/10.1093/oxfordjournals.annonc.a059215
|
| [9] |
Singh D, Roy N, Das SM. Epidemiology, pattern of recurrence and survival in triple-negative breast cancer. Asian Pacific Journal of Cancer Care. 2020 Jun 7; 5(2): 87-94.
https://doi.org/10.31557/apjcc.2020.5.2.87-94
|
| [10] |
Sharma P. Biology and management of patients with triple-negative breast cancer. The oncologist. 2016 Sep 1; 21(9): 1050-62.
https://doi.org/10.1634/theoncologist.2016-0067
|
| [11] |
Taha Z, Eltom SE. The role of diet and lifestyle in women with breast cancer: an update review of related research in the Middle East. BioResearch open access. 2018 May 1; 7(1): 73-80.
https://doi.org/10.1089/biores.2018.0004
|
| [12] |
Von Minckwitz G, Martin M. Neoadjuvant treatments for triple-negative breast cancer (TNBC). Annals of oncology. 2012 Aug 1; 23: vi35-9.
https://doi.org/10.1093/annonc/mds193
|
| [13] |
Payandeh M, Sadeghi M, Sadeghi E, Aeinfar M. Clinicopathology figures and long-term effects of tamoxifen plus radiation on survival of women with invasive ductal carcinoma and triple negative breast cancer. Asian Pacific Journal of Cancer Prevention. 2015; 16(12): 4863-7.
https://doi.org/10.7314/APJCP.2015.16.12.4863
|
| [14] |
Bayoumi Y, AbdelSamie A, Abdelsaid A, Radwan A. Locoregional recurrence of triple-negative breast cancer: effect of type of surgery and adjuvant postoperative radiotherapy. Breast Cancer: Targets and Therapy. 2014 Sep 10: 151-8.
https://doi.org/10.2147/BCTT.S69309
|
| [15] |
Yuniastini Y, Murhan A, Purwati P, Pratiwi MD. Risk factors for breast cancer: hormonal contraception. Jurnal Aisyah: Jurnal Ilmu Kesehatan. 2022 Jul 25; 7(S1): 349-54.
https://doi.org/10.30604/jika.v7iS1.1307
|
| [16] |
Wen S, Manuel L, Doolan M, Westhuyzen J, Shakespeare TP, Aherne NJ. Effect of clinical and treatment factors on survival outcomes of triple negative breast cancer patients. Breast Cancer: Targets and Therapy. 2020 Mar 6: 27-35.
https://doi.org/10.2147/BCTT.S236483
|
Cite This Article
-
APA Style
Nahar, S., Anika, A. S., Majumder, R. A., Akhter, K., Ahmed, F., et al. (2025). Assessing the Impact of Chemoradiotherapy and Surgery on 2-Year Survival of Triple Negative Breast Cancer Patients- A Prospective Follow-Up Study. International Journal of Clinical Oncology and Cancer Research, 10(2), 59-66. https://doi.org/10.11648/j.ijcocr.20251002.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Nahar, S.; Anika, A. S.; Majumder, R. A.; Akhter, K.; Ahmed, F., et al. Assessing the Impact of Chemoradiotherapy and Surgery on 2-Year Survival of Triple Negative Breast Cancer Patients- A Prospective Follow-Up Study. Int. J. Clin. Oncol. Cancer Res. 2025, 10(2), 59-66. doi: 10.11648/j.ijcocr.20251002.13
Copy
|
Download
AMA Style
Nahar S, Anika AS, Majumder RA, Akhter K, Ahmed F, et al. Assessing the Impact of Chemoradiotherapy and Surgery on 2-Year Survival of Triple Negative Breast Cancer Patients- A Prospective Follow-Up Study. Int J Clin Oncol Cancer Res. 2025;10(2):59-66. doi: 10.11648/j.ijcocr.20251002.13
Copy
|
Download
-
@article{10.11648/j.ijcocr.20251002.13,
author = {Shamsun Nahar and Afsana Sharmin Anika and Rumana Afroz Majumder and Khursheda Akhter and Faruk Ahmed and Nasrin Akhter and Fariha Chowdhury and Saimum Islam},
title = {Assessing the Impact of Chemoradiotherapy and Surgery on 2-Year Survival of Triple Negative Breast Cancer Patients- A Prospective Follow-Up Study
},
journal = {International Journal of Clinical Oncology and Cancer Research},
volume = {10},
number = {2},
pages = {59-66},
doi = {10.11648/j.ijcocr.20251002.13},
url = {https://doi.org/10.11648/j.ijcocr.20251002.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcocr.20251002.13},
abstract = {Triple-negative breast cancer is a rising concern recently as incidence and deaths have doubled within two years. Despite various proven risk factors and effective therapies, improvements in survival rates have not been up to the mark. This study evaluated 110 patients with histologically proven stage I-III TNBC with invasive ductal carcinoma treated from 2021 to 2023, all of whom underwent surgery, chemotherapy, and radiotherapy. The majority of patients were over 35 years old (69.1%, median age 40±10.6 years), with left-sided cancers being more common (60%), and mastectomy was the primary surgical approach (76.4%), often followed by adjuvant chemotherapy (88%). The most prevalent tumor size was T2 (88.2%) and nodal status was N1 (52.7%), with T2 and N1 showing significant prevalence across surgical and chemotherapy groups; recurrence was higher in patients receiving neoadjuvant chemotherapy and lumpectomy, while survival was higher with mastectomy compared to lumpectomy and with adjuvant versus neoadjuvant chemotherapy. The findings suggest that adjuvant chemotherapy and mastectomy with radiotherapy have a significant effect on the 2-year survival of TNBC patients in this cohort, reinforcing the prognostic importance of tumor stage and nodal involvement. This may have a vital role in the prognosis of the disease and has a huge scope for research.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Assessing the Impact of Chemoradiotherapy and Surgery on 2-Year Survival of Triple Negative Breast Cancer Patients- A Prospective Follow-Up Study
AU - Shamsun Nahar
AU - Afsana Sharmin Anika
AU - Rumana Afroz Majumder
AU - Khursheda Akhter
AU - Faruk Ahmed
AU - Nasrin Akhter
AU - Fariha Chowdhury
AU - Saimum Islam
Y1 - 2025/04/22
PY - 2025
N1 - https://doi.org/10.11648/j.ijcocr.20251002.13
DO - 10.11648/j.ijcocr.20251002.13
T2 - International Journal of Clinical Oncology and Cancer Research
JF - International Journal of Clinical Oncology and Cancer Research
JO - International Journal of Clinical Oncology and Cancer Research
SP - 59
EP - 66
PB - Science Publishing Group
SN - 2578-9511
UR - https://doi.org/10.11648/j.ijcocr.20251002.13
AB - Triple-negative breast cancer is a rising concern recently as incidence and deaths have doubled within two years. Despite various proven risk factors and effective therapies, improvements in survival rates have not been up to the mark. This study evaluated 110 patients with histologically proven stage I-III TNBC with invasive ductal carcinoma treated from 2021 to 2023, all of whom underwent surgery, chemotherapy, and radiotherapy. The majority of patients were over 35 years old (69.1%, median age 40±10.6 years), with left-sided cancers being more common (60%), and mastectomy was the primary surgical approach (76.4%), often followed by adjuvant chemotherapy (88%). The most prevalent tumor size was T2 (88.2%) and nodal status was N1 (52.7%), with T2 and N1 showing significant prevalence across surgical and chemotherapy groups; recurrence was higher in patients receiving neoadjuvant chemotherapy and lumpectomy, while survival was higher with mastectomy compared to lumpectomy and with adjuvant versus neoadjuvant chemotherapy. The findings suggest that adjuvant chemotherapy and mastectomy with radiotherapy have a significant effect on the 2-year survival of TNBC patients in this cohort, reinforcing the prognostic importance of tumor stage and nodal involvement. This may have a vital role in the prognosis of the disease and has a huge scope for research.
VL - 10
IS - 2
ER -
Copy
|
Download